|
Article written by: Sharon Kitchen- Clinical aromatherapist and massage therapist at The West-Gate Clinic  Despite the onset of menopause hitting women around the world at a similar age, usually 49/50 years old, why do Japanese women experience menopausal symptoms less than western women? If your mind springs to genetic factors, think again. When Japanese women move to western countries, research has found that their symptoms increase. Dr. Mary Jane Minkin, a professor in obstetrics, gynecology and reproductive health at Yale Medical School believes that the answer lies with the social perception of aging. Women are thought of as wiser and more respected with age in Japanese culture, with the menopause often being embraced as a positive life event. The perception in the western world can often be the opposite, with age and the menopause combining, leading to fear, catastrophisation and the beginning of a downward spiral. There is also the western inclination to place a high importance on the value of youthfulness. We only have to see the amount of Botox pumped into faces to try and banish wrinkles and lines to understand that the obsession with youthfulness is appearing in women way before the onset of the menopause. Attitudes toward the menopause are not inflexible, in fact research reports that negative attitudes towards the process can act as a “Self Fulfilling Prophecy” resulting in women who have a neutral or positive attitude to this transitional phase having a very different experience. So how could menopause be seen as a good thing? Well the results of menopause can offer sexual freedom, freedom from the need of contraception and also financial pressure on the purchase of sanitary wear. Menopause in the western world is largely medicalised and dominated by terms such as “reproductive failure” and “ovarian failure” giving rise to the attitude that menopause is a disease that must be treated rather than a biological transition. The Continence Foundation of Australia reports that In the Arab world, the word menopause corresponds to the period in life meaning “desperate age”. Yet native American women don't have a single word meaning menopause and Japanese women have no equivalent word for hot flushes. In some Islamic and African societies post menopausal women no longer have to observe strict gender rules which could account for lower reported symptoms. Looking solely at Japanese culture has produced two examples of non medical influence on menopause. Social context, paired with diet. Therefore, as with obesity, heart disease, depression and anxiety, there’s a solid argument for natural interventions and lifestyle changes to lead the way before automatically choosing the mainstream medical route of HRT. So is it solely a social predicament? As well as Japanese women reportedly suffering less severe hot flushes, they have also been shown to have a lower risk of vascular disease, osteoporosis and brain cancer. One of the theories that links these symptoms together is that Japanese women include a lot of Soy in their diet which contains isoflavones. Isoflavones are naturally occurring molecules that can be found in various beans. They have been found to increase the serum oestrogen levels in people who have a high content of these beans in their diet. Isoflavones can also be taken as a supplement. Low bone density is one of the main downsides of the menopause, which is why a 2020 paper conducted a systematic search of soybean influence on menopausal bone density changes. The study found that ‘Isoflavone interventions, genistein (54 mg/day) and ipriflavone (600 mg/day) in particular, have beneficial effects on bone mineral density outcomes and are safe in postmenopausal women’. References
https://www.continence.org.au/news/cultural-perspectives-menopause https://pubmed.ncbi.nlm.nih.gov/32524173/ https://www.reuters.com/article/us-health-menopause-perceptions-idUSKBN0OL1XH20150605 https://bmcwomenshealth.biomedcentral.com/articles/10.1186/1472-6874-12-43
0 Comments
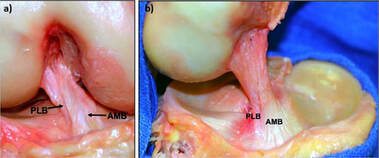
What is the anterior cruciate ligament?The ACL is a major structure of the knee and is commonly associated with sporting injuries. The ligament attaches from the femur (thigh bone) to the tibia (shin bone). The ACl is made up of thick wavy bundles of collagen fibres. These fibres are aligned in a variety of directions and orientations all aimed at providing integrity, tensile strength and resilience to the forces imposed upon it. These lines of orientation make it different to other ligaments of the body and a perfect example of adaption to the stresses the knee has taken throughout it's evolution. The two major bundles are known as the anteromedial bundle (AMB) and the posterolateral bundle (PLB). The role of the AMB is to prevent the tibia (shin bone) from excessive anterior translation. This basically means if the AMB wasn't present, the shin bone would be able to slide forward of the femur (thigh bones). An image of what this tibial translation look like in real life can be seen below. The PLB is a larger bundle and this has the role of stabilising the joint during rotational pivot like movements. As well as these alternate roles, they also tighten during different movements too, as if to cover one another for possible excessive movements. The AMB typically tightens during flexion of the knee (Bringing your heel to your bum or squatting), whereas the PLB tightens during extension of the knee (jumping or standing upright).
The general purpose of the ACL is to provide stability of the knee and prevent that anterior tibial translation. The knee under goes huge forces on any given day. These forces can sometimes be taken for granted. For example, forces translated through the knee joint during walking have been measured to be between 2-3 times bodyweight. This is somewhere up to 240kg for the average 80kg male, and that's just from walking. This highlights the importance of trying to keep within a healthy weight for your height. For every kg of bodyweight gained and extra 2-3kg is being sent through the knee every step. The design of the knee is complex. Not only do the articular surfaces (touching surfaces) of the femur have to move perfectly with the articular surfaces of the tibia, but the muscles attaching to the knee also have to behave in a fashion that supports proper alignement and force distribution. These muscles also attach to other joints such as the hip and ankle, where the joint dynamics also need to be efficient. We've all had examples of suffering an injury and a joint above or below taking the brunt. Like rolling your ankle and slowly developing knee pain. This is usually due to complex compensation patterns occurring between joints and muscles of both sides of the body. It's been found that only 3-5 degrees of increased varus on the knee (Knees moving outward bowing away from one another as shown below), can result in a 50% increase in the force transmitted across the medial tibiofemoral compartment. 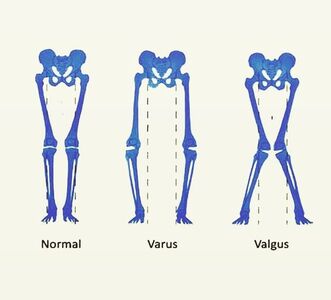 Mechanisms of injuryBy mechanism of injury we mean 'what are the usual things that cause damage to the ACL'. We'll also discuss predisposing factors here too. Although the ACL is commonly injured in sport, it's most commonly the non contact aspect of sport that does the damage. 70% of ACL injuries are non contact. Sports such as basketball, football and rugby, which require a frequent amount of pivoting are all main contributors of ACL tears. One difficulty in a clinical setting is differentiating between a meniscal tear (the cartilaginous shock absorbers of the knee) and an ACL tear, due to both having similar mechanisms of injury, both creating instability in the knee when torn and both resulting in a possible popping sound. Another reason athletes frequently injure the ACL, is lack of hamstring strength, or the ratio between hamstring and quadricep strength being insufficient. As stated, the ACL prevents anterior translation of the tibia, the hamstrings also do this due to their attachment points at the back of the knee. This statement from a study by Myer et al. 2009 sums it up. 'There is evidence showing that female athletes who suffered an ACL injury subsequent to strength testing, had reduced hamstring but not quadriceps strength and conversely, those who did not go on to ACL injury had adequate hamstring strength'. Deceleration is also a mechanism of injury. Next time you watch the 100m or 200m sprint, notice how the runners continue to run for another 30 or so metres before coming to a steady halt. They don't rush this as its the most likely time to rupture a quadricep muscle, or cause stress damage to the ACL. The large quadriceps of sprinters are powerful enough to drag the tibia anteriorly as they attempt to slow the body down. This paired with the shearing force of decelerating at a fast pace is enough to sustain damage over time. The opposite is true for the hamstrings which will be covered in future blog posts. Acceleration is the usual mechanism of injury for hamstring tears. Females are up to 3 times more likely to suffer with an ACL rupture. Not very fun if you're a woman, but the reason for this is something called a 'Q angle'. The Q angle is shown in the image below. It highlights the difference between a typical male and female Q angle. The reason for this is to accommodate for a wider female pelvis. The hips are wider set which as a result increases the Q angle. As discussed earlier in regards to joint orientation increasing the stress placed on a joint, it's clear to see that the large angle would alter and increase the lines of stress through the joint and ACL and reduce force distribution. This further increases the need for females to increase their hamstring strengthening work particularly if they play high level sport. 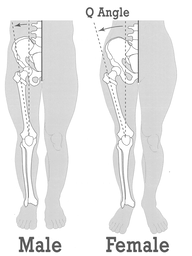 Contact and the unhappy triadThe unhappy triad may sound like a star wars spin off, but it actually refers to three injuries commonly seen together and usually caused from direct contact to the leg on a planted foot, common in football sliding tackles. The tibia (shin bone) is forced into a valgus position as shown above, whilst the foot remains planted to the floor. This usually puts enough pressure through the knee to cause damage to the following; ACL, medial meniscus and medial collateral ligament. This is crucial to both pitch side and clinical diagnosis. Suspecting injury of one of these structures after a contact injury should raise the question of the state of the remaining 2 structures. 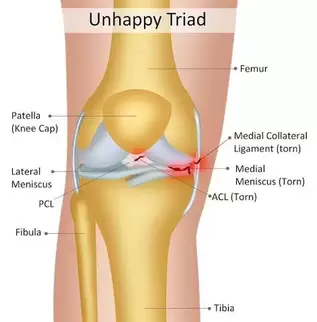 The ACL's role in proprioceptionAs well as being movement preventors and joint stabilisers through their structure. Ligaments such as the ACL are also proprioceptive aids. In short, they send signals to the spinal cord to alert the nervous system where the joint is in space and time. If you close your eyes and get someone to flex or extend your fingers, the ligaments are the things letting your body know what position the joint is in. Notice how you don't need to open your eyes to find out. This is the same with the ACL, every time we walk, jump, slip, squat etc the ACL is sending thousands of signals to your nervous system continuously. The faster and more efficiently these signals are sent, the safer the joint is and the quicker the reaction time to external stimulus like ice under foot or an opposition player coming in for a tackle. A meta analysis in the journal of physiotherapy found that when practitioners used a joint position test and threshold to detect passive motion testing, injured ACL individuals performed worse than those uninjured. The reliability and validity of these testing methods were noted to be questionable, however it highlights the role the ligament plays in balance. Grades of tearGrade 1- Stretching of the ACL as a result of excessive force but no tear. Little tenderness and swelling, no joint laxity. Grade 2- A partial tear of some of the ligament fibres, some laxity shown with possible giving way, Lachman's and anterior drawer tests positive for pain but still have a firm end feel. Grade 3- A full rupture, all fibres of the ligament have torn in 2. Probably swelling, extreme instability, soft end feel on testing. Bleeding into the joint present (hemarthrosis). 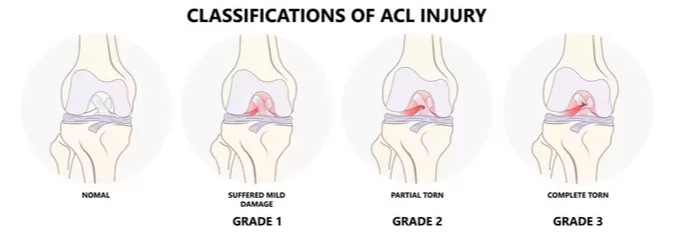 West-Gate uses two orthopaedic tests to assess ACL damage. These are known as the anterior drawer test and the Lachman's test. Although these tests can be useful particularly when accessing high grade 2 and 3 tears for joint laxity. Most diagnosis come as a result of what the patient says during our case history and initial questioning. Onset of injury (traumatic, popping heard, giving way etc) gives us as osteopaths and sports therapists, the indication of level of injury. The psychology of it all. Dark places, finances and loss of identityOne of the biggest issues with ACL injuries is the effect it has on an individuals mentally. Some individuals depend on their knee to continue working or competing. There's plenty of examples of people relying on reduced sick pay throughout their recovery or being dropped from highly competitive sports clubs. If you're an athlete and your whole life is sports orientated (hobbies, circles of friends, stress relief etc), then you lose all aspects of your identity throughout the recovery process. This is why if it's noticed that a patient is suffering from the mental aspects of recovery, counselling is often encouraged. Some fantastic resources to utilise when recovering from an ACL sprain or rupture, include accounts written by people who have managed to successfully recover and return to sport, injury support groups on social media and a good osteo, physio or sport therapist to encourage you and guide you through the process. Personal injury insurance that covers you for out of work incidence is also worth looking into if you participate in high risk activities. Post surgery methods. Conservative or acceleratedThere are two main approaches to returning to sport after ACL reconstructive surgery, conservative and accelerated. The conservative approach suggests a return to sport at least 9 months post surgery. The accelerated approach aims at returning individuals within 6 months. Bare in mind that regardless of approach, only 55% of individuals return to competitive sport. Requirements to returning to sport carried out by healthcare practitioners such as osteopaths, physiotherapists and chiropractors used to be mostly time based e.g. after 1 year. More recently that changed to a check list approach of tasks to complete before return such as equal quad and hamstring strength, equidistant single leg jumps between repaired and uninjured sides. This almost sounds more sensible, if the individual can carry out tasks equal to the uninjured side and appears to have a knee just as able and athletic as the other side, why not return to sport? Well in turns out, time may play a more vital role than first anticipated. Revascularisation is one of the main advocates of the conservative approach. Waldron. et al 2022 analysed ACL reconstruction research papers and found that although many aspects of the reconstruction heal and regain full capabilities within 6-9 months, it takes the surgical graft 12 months or more to fully regain its vascularity. Without blood, the area can't heal and repair efficiently. The inner rings of the knees meniscus is a perfect example of this. The authors also found that 'there is some evidence that reinjury incidence is reduced by 51% per month for each month that return to sport is delayed' between 5-9 months post surgery. Here's another terrifying research paper title for you; 'Young athletes who return to sport before 9 months after anterior cruciate ligament reconstruction have a rate of new injury 7 times that of those who delay return'. (Beischer. et al 2020). The accelerated method takes a modern approach to rehab. It promotes immediate weightbearing of the reconstructed ACL and discourages the use of braces and walking aids. This is smart as initial ligament laxity and instability post surgery has shown to have absolutely no correlation between reinjury in both conservative and accelerated approaches, highlighting the fact that the knee can be safely loaded days after surgery. The accelerated approach obviously has its benefits such as returning to sport faster, reducing muscle wastage and improving the mental wellbeing of an athlete intending to return to sport. Theoretically... unfortunately as ideal as the accelerated approach appears, nothing can counteract the statistics stated above in regards to reduction of reinjury rate per month post surgery and the revascularizing needs of the surgical graft. As a result of the evidence, the West-Gate clinic takes a blended approach to rehabbing the ACL post surgery. Weightbearing and movement is encouraged after surgery as stated in the accelerated approach, however a return to sport is discouraged up until the 9-12 month stage, where testing for the specific capabilities is carried out on a pass fail basis. Some of the clinics testing requirements are shown below. 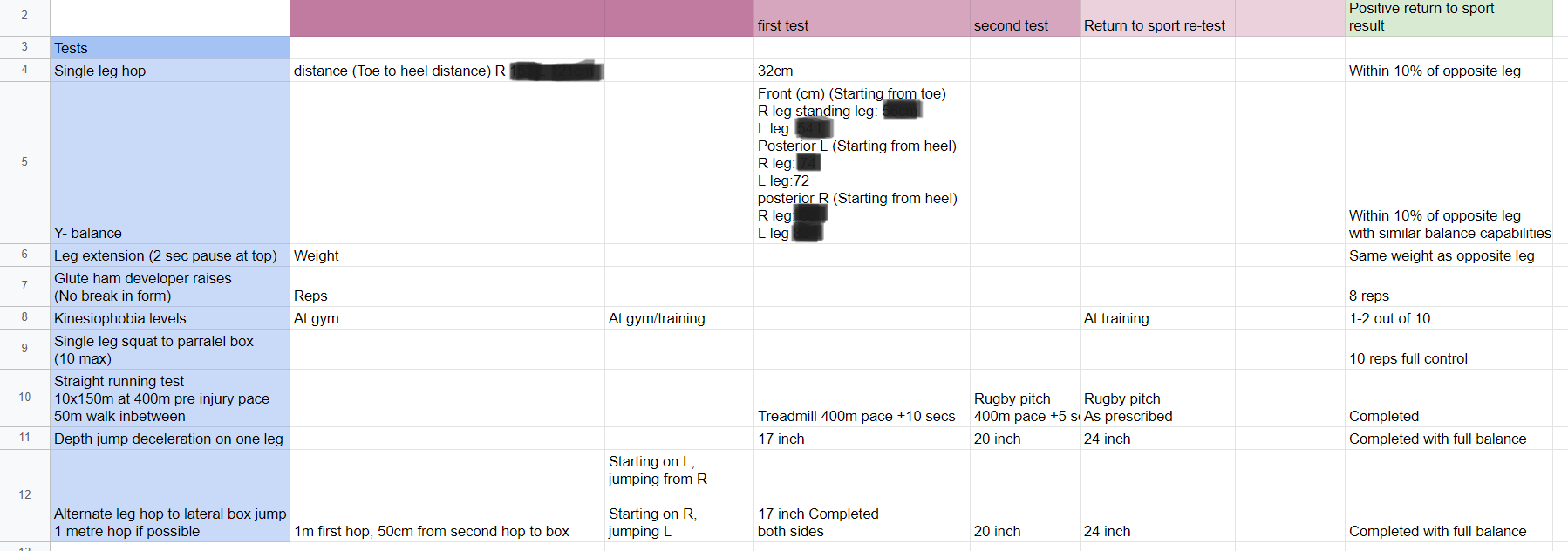 5 steps patients at the clinic undertake: - Surgery recovery, weightbearing, walking and leg straightening - Neuromuscular control - Running and agility - Returning to sport - Prevention of reinjury Prevention of injurySo what can be done? Occasionally in sport, injuries are unavoidable, particularly in a sport contact sense as described above with forceful impact injuries. However, things can be done to combat repetitive strain and reduce stress on the joints. The 'prevention is better than cure' approach should always be taken whether you play sport or not. Therefore, hamstring work is our first bit of advice. Hamstring strengthening for real world application should include, isometric and eccentric loading. Think about how these apply particularly to sport. If you're a sprinter, the hamstrings have to contract hard from a lengthened position, making eccentrics valuable. Wrestlers and jiu jitsu fights may have prolonged periods of time in a bent over stance, which would benefit from the use of isometric holds. Proprioceptive exercise will benefit not only the ACL, but all the other ligaments of the knee and ankle. These exercises will increase the speed and fluidity of the signals being sent back to the spinal cord telling the nervous system where the joint is in space and time. This quicker signalling results in a faster return signal and action. It can be the difference between successfully correcting of a movement and being too late. Most efficient exercises to strengthen the hamstrings in different positionsThe Romanian deadlift- This movement can be performed in a variety of way for a variety of reasons. Using single leg varieties and deficits to enhance the effectiveness can be useful. It allows the hamstrings to be heavily loaded whilst being lengthened under control. Adding pauses and strength training tempos can also add a new dynamic to the movement. Glute hamstring curls or nordics- These movements in their purest form are an advanced exercise. They take a level of strength only achievable by someone who has good quality strength and control over their hamstrings already. Therefore, we need to use progressions to get to this point. Try performing a nordic with a box in front of you to push off and simply lower yourself to the point you can hold no longer, as slowly as possible, then use your arms to push yourself back up. If you get comfortable with these and have access to a glute ham developer machine, take advantage as it's a brilliant piece of kit.
Most efficient proprioceptive exercises for the ACL and ligaments of the knee The depth jump to single leg landing- Standing on a small box up to 20 inches for those who are confident and adept at jumping. Step forward off the box landing and springing immediately back up using both feet to a box of the same height. Land with one leg, stabilise yourself, then repeat on the other leg. This exercise not only enhances the proprioception of the knee and ankle ligaments on take off and landing, it also adds to that spring load effect we look for in healthy tendons. Bosu ball throw and catch- Standing on a Bosu ball or balance board with one or two legs depending on confidence and ability. Throw a ball at a wall 2 feet away and catch it again. Repeat this on one leg if successful on both. Contact specific proprioception- The above exercises are great for general proprioception in non contact sports. However, sports such as rugby or American football need more contact stimulus. This could include introducing controlled contact by a training partner or coach whilst jumping and landing. Meaning to knee gets used to fast changes of unpredictable direction. References- R Strocchi, V de Pasquale, P Gubellini, A Facchini, M Marcacci, R Buda, S Zaffag. (1992). The human anterior cruciate ligament: histological and ultrastructural observations.. Journal of anatomy. 181(-), p.521.
- Jay R Ebert, Peter Edwards, Peter T. Annear. (2022). Selective bundle reconstruction for symptomatic partial anterior cruciate ligament tears demonstrates good functional sc. The knee. 36(-), pp.53-64. - Susanne Beischer, Linnéa Gustavsson, Eric Hamrin Senorski. (2020). Young Athletes Who Return to Sport Before 9 Months After Anterior Cruciate Ligament Reconstruction Have a Rate of New In. Journal of orthopaedic & sports physical therapy. 50(2), pp.83-90. - Kristen Waldron, Matthew Brown, Ariana Calderon, Michael Feldman. (2022). Anterior Cruciate Ligament Rehabilitation and Return to Sport: How Fast Is Too Fast?. Arthroscopy, sports medicine and rehabilitation. 4(1), pp.175-179. This week alone we've had two patients present to clinic with a potential spondylolisthesis. So what is it? Is it dangerous, can it be seen or felt? You can't slip a disc like people will tell you, but you can slip a vertebral joint. Here's how. Spondylolisthesis refers to the forward slippage of a vertebral joint of the spine due to a fracture of something called the ‘pars interarticularis’. Spondylolysis is the stage preceding spondylolisthesis, where the pars has either weakened or has stress fractured, but no slippage has occurred. If this fracture is severe and unstable, the vertebral joint is able to slide forward as its no longer 'locked in' by the pars. Leading to the condition known as spondylolisthesis. You can see these three stages below. Look out for the pars in the diagram and how it would work to prevent the joint below it slipping outside of its normal range. It acts almost like a jigsaw puzzle, fitting nicely with the joint below. 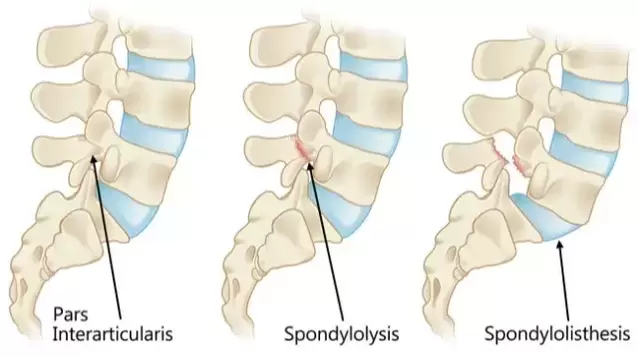 Most commonly, spondylolisthesis affects the lumbar spine (low back) due to the curvature of the spine and the fact that it's the most weight bearing region. However, it can be seen in the neck and thoracic spine.
It can be caused by traumatic injury, typically some sort of hyperextension injury of the low back e.g. gymnastics fall or car accident. However, more commonly it's caused through repetitive stress or degeneration of the pars described above. A spondylolisthesis is graded depending on the severity of the forward slippage. There are four grades as shown below. These gradings are important as it alters prognosis and instability within the spine. Natural selection acts solely by accumulating slight successive favourable variations, it can produce no great or sudden modification; it can act only by very short steps. - Charles Darwin Structure governs functionDuring my time at university, I was introduced to the principle "structure governs function". In anatomical terms, this means that our bodies developed in a way that serves a specific, necessary ability e.g. 4 fingers and a thumb which allow humans to grip, use tools and illustrate hand signals as communication. I use the word necessary intentionally. Darwin's theory of evolution by natural selection tells us the long term changes to anatomy and physiology only occur when they give an organism an advantage, therefore being deemed necessary. There was always debate amongst my peers and lecturers on whether this principle can be flipped around; "function governs structure". In the short term, yes. When a person permanently loses a sense, for instance hearing, it's common knowledge that the remaining senses often become heightened. A study published in the Journal of neuroscience in 2012 found that when the brains of congenitally deaf people were observed through fMRI (A fancy MRI scanner that allows activity of the brain to be monitored), the researchers found that rather than the area of the brain that is in charge of hearing (Heschl's gyrus) being missing or empty, it's role had been altered through the process of neuroplasticity to detect vision and touch. However, this trait is not passed on through reproduction and the function of the parents advantageous vision and touch has not altered the structure of their child's Heschl's gyrus. The reason for this is summarised in the Darwin quote at the top of this page. Permanent changes to anatomy only occur over extremely long periods of time, in tiny incremental progressions. Therefore, it doesn't appear that function can govern structure, particularly in the short term in a way that will positively adapt a human being to a new day to day lifestyle. This, I believe is the underlying issue of modern societies battle with pain, stiffness and disease. It gives a reason as to why our bodies don't suddenly alter themselves to suit our office jobs, evenings slumped on the sofa, diets dense in processed foods and the 3-4 hours UK adults spend on average watching television every day.  Why we've decided to write a blog and an introduction to the teamThe West-Gate clinic was given a new lease of life in February 2022. Becky and Niall, then associate Osteopaths at West-Gate, decided to undertake the challenge of managing the clinic and developing it to such a level that it provides a critical multi-disciplinary role in the community. It's common knowledge that our NHS counterparts are seeing an overwhelming amount of patients and that resources, money, staff and time is having to be rationed at the expense of the British public. Therefore, as a healthcare practice, we believe it's our responsibility to provide a private option for the people of East Yorkshire. With this in mind, The West-Gate clinic needed to be multi faceted. We didn't want to focus solely on physical health, or injury. Health and injury is as much about lifestyle factors, mental wellness and education as is it about everyday musculoskeletal conditions. As a result, we now have a wonderful team of practitioners trained in an array of different healthcare practises, enabling The West-Gate clinic to provide competent health assessments, treatments and follow up advice. The clinic is now easier to access than ever, with online bookings now available on the website www.thewestgateclinic.com. Telehealth video appointments will shortly become available with Osteopath Nick Brown which will allow patients to speak to an MSK specialist from the comfort of their own home.  So who are we? |
AuthorsNiall Walsh Archives
July 2023
Categories |

 RSS Feed
RSS Feed

|
|
|
|