|
This week alone we've had two patients present to clinic with a potential spondylolisthesis. So what is it? Is it dangerous, can it be seen or felt? You can't slip a disc like people will tell you, but you can slip a vertebral joint. Here's how. Spondylolisthesis refers to the forward slippage of a vertebral joint of the spine due to a fracture of something called the ‘pars interarticularis’. Spondylolysis is the stage preceding spondylolisthesis, where the pars has either weakened or has stress fractured, but no slippage has occurred. If this fracture is severe and unstable, the vertebral joint is able to slide forward as its no longer 'locked in' by the pars. Leading to the condition known as spondylolisthesis. You can see these three stages below. Look out for the pars in the diagram and how it would work to prevent the joint below it slipping outside of its normal range. It acts almost like a jigsaw puzzle, fitting nicely with the joint below. 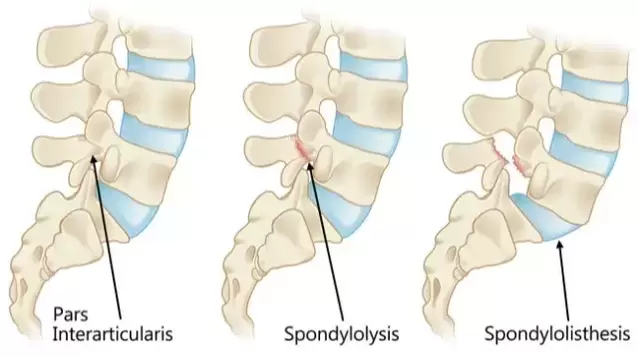 Most commonly, spondylolisthesis affects the lumbar spine (low back) due to the curvature of the spine and the fact that it's the most weight bearing region. However, it can be seen in the neck and thoracic spine. It can be caused by traumatic injury, typically some sort of hyperextension injury of the low back e.g. gymnastics fall or car accident. However, more commonly it's caused through repetitive stress or degeneration of the pars described above. A spondylolisthesis is graded depending on the severity of the forward slippage. There are four grades as shown below. These gradings are important as it alters prognosis and instability within the spine.  Varying on the severity of the forward slippage, spondylolisthesis can be diagnosed by your osteopath or physiotherapist as long as they palpate the spinous process of the low back. Making their way down the spine, they should be able to identify a ‘palpable step’. This step is identified by following the intact spinal column down by feeling for the spinous process that has slipped forward, leading to what’s felt as a dip in the spine. Is it dangerous? Spondylolisthesis is fairly common. Estimates suggest it may affect 1 in 20 adults. In a lot of cases, the spine slips forward and the muscles, ligaments, and fractures heal around the new anatomy. Making the spine stable and secure again. These may go undiagnosed for a long period of time, sometimes only found after having an x-ray for an unrelated issue. These undetected cases tend to be of those graded 1-2. Anything pushing towards grade 3-4 are likely to cause some neurological issues (weakness, numbness, pain, pins and needles etc). If you notice anything like this, it’s worth a consultation with your osteo, physio or GP. They will conduct a neurological assessment and should also palpate the spine for obvious symptoms of conditions like spondylolisthesis. To throw a spanner in the works. There is a similar condition with a slightly different mechanism of injury called a retrolisthesis. This condition is the opposite to spondy, where the vertebral joint slips backward, rather than forward. It’s not a common injury and the same rules apply as spondylolisthesis. Get it diagnosed by an expert which may involve an X-ray to highlight the severity. When should I get seen?As with most conditions, the earlier the injury is assessed, the quicker and treatment plan can be put into place. If you experience any neurological symptoms as discussed above. This includes sciatic type symptoms, pains in your glute muscles, weakness of the limbs etc, its worth booking an appointment. The severest of these symptoms is what's known as 'cauda equina'.. This is where the lowest nerves of the spine which control a persons saddle region are affected. This can lead to incontinence and a full weakness of the lower limb. If this is experienced, it's a medical emergency and an ambulance should be called. This is however rare. What can be done?In most cases, physical therapy provided by an osteopath or physiotherapist is adequate to strengthen and stabilise the spine. Remember, the spine is far from a fragile structure. It has thick ligaments binding it together, shock absorbing intravertebral discs cushioning forces running up and down it and a thick layer of muscles interlinked amongst it's joints and layered behind it to provide protection, stability and movement. These are the structures which the spine will depend on if it's compromised through spondylolisthesis. At your appointment, you will also be advised on movements to avoid. These will include things like large extension movements seen in gymnastics and yoga as well as excessive stretching of the spine. In severe cases, surgery may be advised by a consultant to fuse the joints together to prevent further slippage an narrowing of the various vertebral foramina where the nerves are. Spinal decompression is also sometimes used.  If you'd like an appointment you can book online here and follow the link for an osteopathy initial consultation with any of our osteo's. Alternatively, if you're not in the UK or can't get to the clinic, our telehealth online appointments can be viewed here. You'll have access to one of our osteo's through a video call and the same follow up care you'd receive if you attended the clinic. 
0 Comments
Leave a Reply. |
AuthorsNiall Walsh Archives
July 2023
Categories |
 RSS Feed
RSS Feed

|
|
|
|